Main » Scientific articles » The latest method of enamel remineralization using high-intensity focused ultrasound
The latest method of enamel remineralization using high-intensity focused ultrasound
Remineralization is a crucial interventional strategy for preventing white spot lesions (WSL) of the enamel. Given the limitations of both natural and/or fluoride-mediated repair processes, there is a need to develop new strategies for the restoration of WSL using a minimally invasive approach that restores the unique ultrastructural integrity and functional properties. Inspired by the unique ability of high-intensity focused ultrasound (HIFU) to accelerate the crystallization process, we propose a new strategy of utilizing HIFU for the restoration of WSL in vitro through the synergy of the crystallization process necessary for the formation of hydroxyapatite (HAP) from its precursor (calcium phosphate ion clusters; CPIC).
After the development and characterization of CPIC, including the obtained amorphous calcium phosphate (ACP), the influence of HIFU on the transition of ACP to HAP on an amorphous substrate was investigated using transmission electron microscopy and high-resolution transmission electron microscopy, selected area electron diffraction, and X-ray diffraction (XRD). The results showed a profound amorphous-crystalline phase transition within 5–30 minutes of HIFU exposure.
Subscription Membership Required
You must be a Subscription member to access this content.
To restore the enamel, artificial WSL were created on enamel samples, followed by HIFU exposure for 2.5, 5, or 10 minutes. Scanning electron and atomic force microscopy revealed a reduction in surface roughness and the gradual erosion of the porous structure of WSL with continuous linear coaxial alignment of HAP crystallites filling the prismatic/interprismatic gaps, closely resembling healthy enamel, especially after 5 minutes of HIFU exposure. The ultrastructural restoration of the WSL enamel was further confirmed by XRD spectral analysis with corresponding restoration of mineral density and nanomechanical properties, as reflected in the micro-computed tomography (CT) results. Micro-CT further confirmed the subsurface remineralization of WSL with HIFU exposure. Under the same exposure parameters, HIFU demonstrated a powerful anti-biofilm effect against Streptococcus mutans. This study presented a new approach to the remineralization of WSL enamel through the powerful synergy between HIFU and CPIC.
In minimally invasive dentistry, remineralization is an important strategy for treating early carious lesions. Although saliva contributes to natural remineralization, its effectiveness after white spot lesion formation has been questioned. In this regard, fluoride-mediated remineralization has been proposed as a preventive approach. However, there is an increased risk of fluoride toxicity associated with fluoride intake from multiple sources. Furthermore, studies have shown that fluoride-mediated remineralization impairs the mechanical properties of the restored enamel, as it is unable to form ordered mineral crystals. Secondly, the formation of fluorapatite hinders the diffusion of mineral ions into deeper areas of the lesion, leading to incomplete enamel remineralization. Given the limitations of both natural and fluoride-mediated repair processes, there is a need to develop new strategies for the restoration of tooth enamel using a minimally invasive approach that restores the unique ultrastructural integrity and functional properties.
Researchers are actively studying innovative methods for remineralizing the early stages of enamel demineralization, such as the formation of hydroxyapatite (HAP) from amorphous calcium phosphate (ACP) nanoparticles as a precursor, protein/peptide-induced mineralization, and hydrogel-induced remineralization. However, these approaches are implemented under strict conditions, including high temperature and pressure, low pH, technical complexities, and/or high cost, which may limit their widespread application in clinical practice.
Стоит отметить, что кристаллиты ГАП в естественной эмали происходят из предшественников AФК, в частности, состоящих из кластеров Познера (Ca9 [ PO4 ] 6 ) , которые представляют собой ионные кластеры с размером домена приблизительно 0,95 нм). Поэтому кластеры ионов фосфата кальция (КФИК) были предложены в качестве границы минерализации для реминерализации эмали. Несмотря на демонстрацию эпитаксиального роста, восстановление эмали с помощью КФИК может быть клинически нежизнеспособным, поскольку метод кристаллизации требует приблизительно 48 часов инкубации в контролируемых условиях. Кроме того, этот подход был исследован только для восстановления деминерализованных фосфорной кислотой поражений в качестве учебной модели, которая не имитировала фактические ранние кариозные поражения эмали.
High-intensity focused ultrasound (HIFU) has attracted widespread attention in medicine and dentistry as a promising therapeutic method due to its unique interaction with biological tissues and non-pharmacological antimicrobial properties. HIFU represents an intense, focused ultrasonic energy capable of generating acoustic cavitation, leading to both physical effects (such as shock waves and high-speed microjets) and chemical effects (such as the formation of free radical species). These properties have been reported to accelerate crystallization processes by controlling the size and shape of synthesized nanoparticles. Furthermore, sonochemical methods have proven to be promising approaches for the synthesis of HAP nanoparticles due to their ability to enhance the nucleation process and reduce crystallization time. Inspired by the unique ability of HIFU to facilitate the crystallization process with its concomitant potential for non-pharmacological antibacterial action, this work proposes a new strategy based on the concept of using HIFU to synergize the in vitro restoration of WSL enamel after the application of CPIC (Fig. 1). Therefore, the first objective is to evaluate the effect of HIFU exposure on the transformation of non-crystalline ACP into crystalline HAP nanoparticles. The second objective is to investigate the synergistic effect of HIFU and CPIC on the restoration of enamel samples containing artificial WSL. The ultimate objective is to assess the anti-biofilm effect of HIFU against cariogenic bacterial biofilms attached to the enamel surface.
Fig. 1. Schematic demonstration of the proposed concept of high-intensity focused ultrasound (HIFU) potential in synergizing the remineralization process of an artificially simulated enamel carious lesion (white spot lesion; WSL) in combination with calcium phosphate ion clusters (CPIC), as well as the associated non-pharmacological antibacterial biofilm effect. (A) Loss of minerals from the tooth enamel due to pH decrease associated with the acidic oral environment caused by cariogenic bacterial biofilms. (B) Scanning electron microscopy image showing the structure and orientation of hydroxyapatite (HAP) crystallites in healthy tooth enamel. (C) Continuous exposure to an acidic environment leading to mineral loss from HAP, affecting the enamel’s prismatic structure and resulting in WSL formation. (D) Schematic presentation summarizing the proposed dual action of HIFU in synergizing WSL enamel remineralization and eradicating the associated cariogenic biofilm. (E) Acoustic cavitation induced by HIFU leads to chemical and physical effects (including the formation of highly reactive radical particles, shock waves, and microjets), which promote the accelerated formation of HAP crystallites in the presence of CPIC for the restoration of WSL enamel (F). Schematic representation (G) and images obtained by confocal laser scanning microscopy (H) demonstrate the non-pharmacological eradication of cariogenic biofilms attached to the enamel surface due to the mechanical impact of HIFU.
HIFU experimental setup
The HIFU setup consists of a bowl-shaped piezoelectric ceramic transducer (H-115; Sonic Concepts) with a resonant frequency of 250 kHz, operating at a power of 30 W (continuous mode), connected to a polycarbonate contact cone (C-101, Sonic Concepts; Fig. 2). The contact cone (containing degassed water) was used for coupling and transmitting the focused waves to the samples.
Рис.2. Схематическая диаграмма, представляющая экспериментальную установку для исследования синергического эффекта высокоинтенсивного фокусированного ультразвука (HIFU) и кластеров ионов фосфата кальция (КФИК) на реминерализацию эмали, а также характеристика антибиопленочного эффекта HIFU на Streptococcus mutans . (A) Иллюстрация метода создания искусственно смоделированного поражения белым пятном (БПЭ). (C) Нанесение синтезированных КФИК на искусственно созданную эмаль БПЭ с последующим воздействием HIFU с частотой 250 кГц при мощности 30 Вт (непрерывный режим) для оценки синергического эффекта HIFU и КФИК для реминерализации эмали WSL (E. (B, D) Выращивание биопленки S. mutans на эмали WSL с последующим воздействием HIFU в течение различных временных точек (F). (G) Компоненты и насадки HIFU, включая чашеобразный пьезоэлектрический керамический преобразователь с резонансной частотой 250 кГц, прикрепленный к прозрачному поликарбонатному соединительному конусу для акустической передачи, а также технические характеристики преобразователя HIFU (H).
HIFU crystallization potential
The influence of HIFU on the transition of ACP to HAP on amorphous glass substrates was investigated. Distilled water was added to glass vials containing ACP nanoparticles obtained from CPIC. Each vial was placed at the focus and exposed to HIFU for varying durations (from 2.5 to 30 min). The resulting HAP was examined using an X-ray diffractometer (Malvern Panalytical) in the 2θ range. The HAP nanoparticles were analyzed using transmission electron microscopy with energy-dispersive X-ray spectroscopy (TEM-EDS), selected area electron diffraction, and high-resolution transmission electron microscopy.
Synergistic effect of HIFU and CPIC on WSL enamel restoration
For the investigation, human premolars (N = 140) were used after obtaining ethical committee approval. Enamel samples were prepared from the buccal surfaces (4×3×3 mm) using a low-speed diamond saw and polished with silicon carbide discs of ascending grit under water cooling, followed by ultrasonic cleaning for 5 minutes in distilled water. Artificial WSL were created and distributed into 5 experimental groups: HIFU exposure without CPIC nanoparticles (HIFU/-NP), CPIC nanoparticles without HIFU exposure (NP/-HIFU), or CPIC nanoparticles followed by HIFU exposure for 2.5 min (NP/HIFU [2.5 min]), 5 min (NP/HIFU [5 min]), or 10 min (NP/HIFU [10 min]).
The enamel surface morphology was examined using scanning electron microscopy. Scanning with atomic force microscopy (AFM) was performed in semi-contact mode at 25 × 25 µm, after which the surface roughness (Sa) was calculated. X-ray diffraction (XRD) peaks of the WSL enamel samples were first recorded in the 2θ range. Enamel samples treated with CPIC before and after HIFU exposure were re-analyzed to investigate any crystallographic changes. Mineral composition analysis was conducted using Raman microscopy.
To assess mineral density and lesion depth, the enamel samples were scanned using micro-computed tomography. For calculating the mineral density, a phantom in Hounsfield units (HU) was calibrated using the same tube (filled with water; water phantom). The HU values for air and water were set at -1000 and 0, respectively, for calibrating the HU scale in the CTAn software. Subsequently, the mineral density was estimated from the projection dataset, where regions of interest were selected from 3 different areas of the WSL. The lesion depth was further measured from the same region of interest slices.
HIFU anti-biofilm effect
The anti-biofilm effect against Streptococcus mutans was evaluated using confocal laser scanning microscopy (CLSM; Nikon, USA), metabolic activity assays (MTT), and colony-forming units (CFU).
The anti-biofilm activity of HIFU is dependent on the exposure time, as confirmed by studies. The effect of HIFU against S. mutans biofilms is explained by the combined action of acoustic microstreaming, microjets, and shock waves generated by acoustic cavitation phenomena. Furthermore, the antimicrobial effect of HIFU without the use of pharmaceuticals may reduce the likelihood of resistance development, as bacteria have less time to adapt to the stress created by the continuous mechanical wave.
Ultrastructural and crystallographic changes
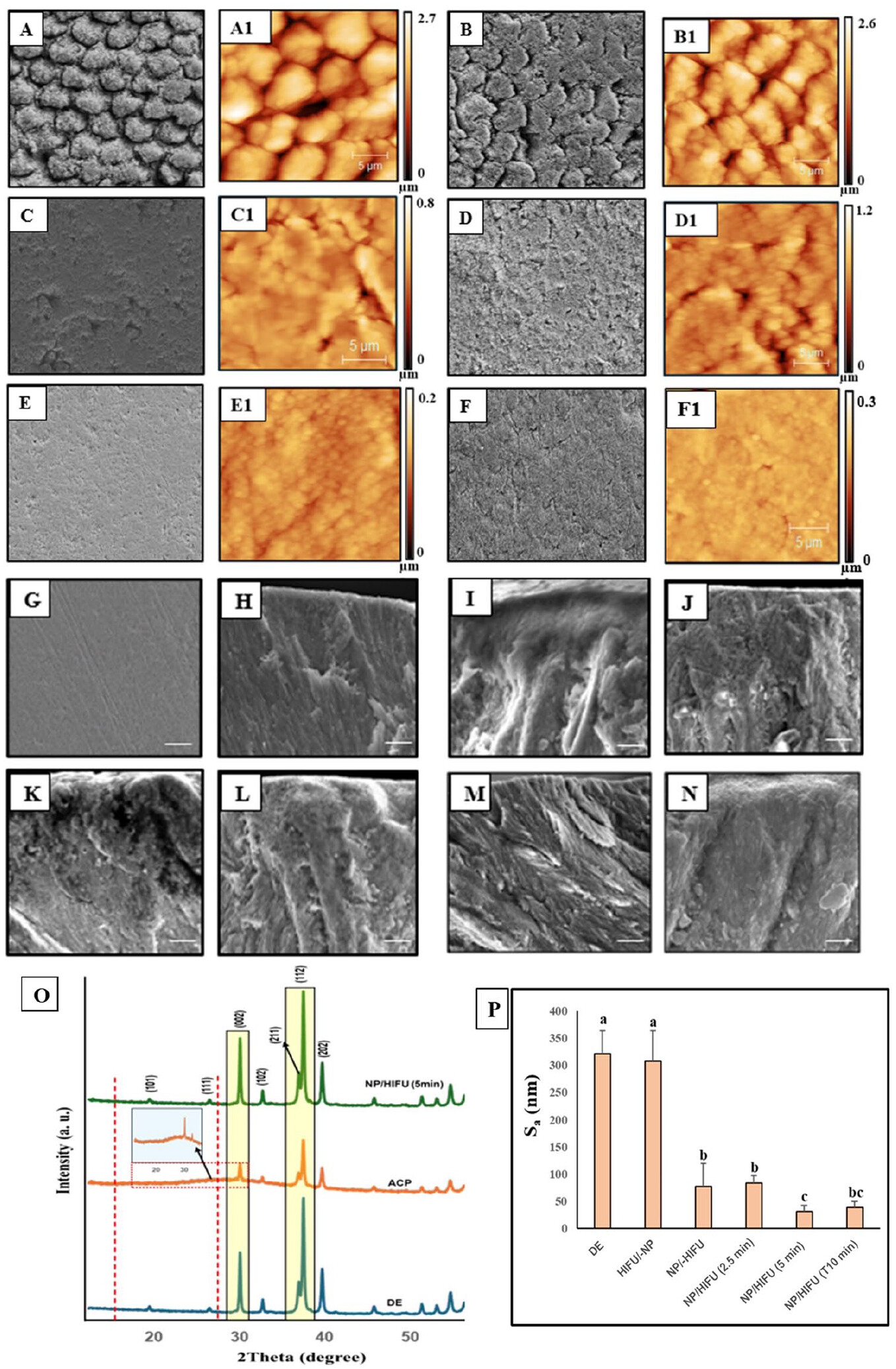
The WSL enamel exhibited a highly porous surface and interprismatic gaps resulting from the loss of HAP crystallites due to mineral ion depletion. This pattern remained unchanged, including the surface roughness, after HIFU exposure (10 min) without the application of CPIC (HIFU/-NP). In contrast, the application of CPIC without HIFU exposure resulted in a smoother surface due to ACP masking the effect of the underlying demineralized porous pattern, as reflected in the X-ray diffraction peak (Fig. 3). After combined CPIC/HIFU treatment, a distinct reduction in surface microporosity, interprismatic gaps, and surface roughness (Sa) was observed with increasing exposure time up to 5 and 10 min. The restoration of the enamel ultrastructure was evident at 5 minutes of HIFU exposure following CPIC application and was comparable to healthy enamel (Fig. 3. E, G, H, M). X-ray diffraction confirmed this finding, revealing a distinct, sharp, intense diffraction peak at 2θ° from 15 to 30° (Fig. 3. O, green spectrum), compared to the broad, low-intensity peak (Fig. 3. O, orange spectrum) recorded in the NP/-HIFU group. This indicates the transformation of ACP (amorphous phase) into HAP (crystalline phase) in the enamel samples treated with CPIC followed by HIFU for 5 minutes.
Fig. 3. (A–G) Images of enamel samples obtained using scanning electron microscopy (SEM) and atomic force microscopy (AFM) (A1–F1).
(A, A1) Enamel with an untreated white spot lesion (WSL) had a highly porous surface and interprismatic gaps. (B, B1) WSL enamel subjected to high-intensity focused ultrasound (HIFU) for 10 minutes demonstrated close morphological similarity to the untreated WSL. (C, C1) Application of calcium phosphate ion clusters (CPIC) alone resulted in a smoother surface texture and the formation of an amorphous calcium phosphate (ACP) coating layer, masking the underlying prismatic and interprismatic structure. Enamel treated with CPIC/HIFU for 2.5 (D, D1), 5 (E, E1), and 10 minutes (F, F1) exposure times, respectively, showed a gradual disappearance of the typical prismatic-interprismatic structure. (G) Healthy enamel. (H–N) Corresponding cross-sectional images of the enamel samples. (H) Healthy enamel, showing a clearly defined, longitudinally oriented prismatic structure with densely packed, rod-like hydroxyapatite (HAP) crystallites extending to the outermost surface layer. (I) The untreated WSL showed a structureless, porous, disorganized surface layer without definite orientation. More or less similar morphological features to the untreated WSL (I) were found after HIFU exposure alone (J), CPIC application alone (K), and CPIC/HIFU exposure for 2.5 minutes (L). A clearly defined, longitudinally oriented prismatic structure with a rod-like morphological appearance was observed after HIFU exposure for 5 minutes (M) and 10 minutes (N) following CPIC application. Specifically, CPIC followed by HIFU exposure for 5 minutes of treatment (M) demonstrated a continuous, organized, linear coaxial arrangement of densely packed HAP crystallites. (O) Spectral analysis of X-ray diffraction (XRD) of the enamel samples. The blue spectrum represents the untreated WSL (DE). Samples treated with CPIC alone (orange spectrum) showed the formation of an amorphous ACP layer, reflected by a broad hump on the XRD pattern at the position 15–30.15° 2θ (inset). However, after subsequent HIFU exposure for 5 minutes (green spectrum), the reappearance of a sharp peak at the same 2θ position suggested the transformation of amorphous ACP into crystalline HAP. (P) The average roughness value (S a ), showing a gradual decrease in surface roughness with increasing HIFU exposure time (error bars represent standard deviation; different letters indicate statistical differences).
It is important to understand that maintaining the long-term integrity of the restored enamel is a complex challenge due to constant episodes of demineralization/remineralization influenced by various factors. Therefore, it is assumed that remineralization using CPIC/HIFU will need to be supplemented with regular oral hygiene. As with any therapeutic intervention, the recurrence of any lesion depends on a number of clinical factors. Therefore, the management of WSL recurrence and/or the emergence of new lesions, which may require re-intervention, is individual and should be considered as part of the patient’s comprehensive treatment plan, including a maintenance phase. HIFU is a non-ionizing, accessible technology that has received several approvals. The installation of miniature transducers on portable devices, such as intraoral scanners, with a set of interchangeable tips featuring different angles is currently being considered. Furthermore, matrix transducers are currently used for applications requiring multiple HIFU exposures on several lesions simultaneously. This facilitates the creation of devices analogous to sectional impression trays, equipped with a set of installed micro-matrix transducers that enable the delivery of HIFU not only to different locations on a tooth but also to multiple teeth simultaneously.
Modern dental practice is undergoing a profound transformation in which digital technologies, interdisciplinary cooperation and access policy play a key
New EFP–EAPD consensus supports age-specific periodontal assessment and management for children and adolescents Introduction / background A joint consensus report
We use cookies to improve website performance, analyze traffic, and personalize content. You can accept all cookies or customize their use. Learn more in our Cookie Policy.
Functional
Always active
Technical storage or access is strictly necessary for the legitimate purpose of making possible the use of a particular service expressly requested by the subscriber or user, or solely for the purpose of carrying out the transmission of a message over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
Technical storage or access used solely for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
Technical storage or access is necessary to create user profiles for the purpose of sending advertising or to track a user across a website or multiple websites for similar marketing purposes.