Main » Uncategorized » Layered modular surgical guides: 1-stage integration of digital workflows and transformation of clinical reproducibility
Layered modular surgical guides: 1-stage integration of digital workflows and transformation of clinical reproducibility
In the era of rapid digitalization, modern dentistry is developing as one of the most dynamic fields of medicine, requiring the integration of digital technologies and clinical practice; in these conditions a key factor of progress becomes not only the development of new devices, but also the effective translation of the digital plan into the surgical field, ensuring reproducibility and predictability of treatment outcomes.
The article discusses the concept of stackable modular surgical guides for full-arch restoration with immediate loading — a description of components, materials, manufacturing approaches and a clinical illustration, analytical reflection on clinical and technological aspects with reliance on evidence-based medicine and digital workflows.
Modularity as a key factor
Stacked modular guides are considered as an element of a unified digital ecosystem that provides mechanical indexing and sequential transfer of implant positions from virtual planning to the operative field; such modularity increases the reproducibility of positioning, simplifies the integration of surgical and prosthetic stages and allows standardization of immediate loading protocols.
Clinical significance lies in the possibility of performing sequential stages — bone reduction, osteotomies, implant placement, fixation of multi-unit abutments and delivery of a provisional prosthesis — within a single digital protocol, which reduces operative time and increases the predictability of outcomes in patients on all-on-X schemes.
Evolution: from static templates to stacked systems
The transition from analog templates to CT- and CBCT-based workflows laid the foundation for stackable modular constructions, since three-dimensional planning and CAD/CAM production allowed the transformation of the guide from an instrument controlling only the angle and depth of drilling into a complex indexing interface for sequential clinical steps.
Technological drivers include the wide dissemination of CBCT, additive and subtractive manufacturing, as well as the integration of photogrammetry and intraoral scanning — all of which reduce barriers to the adoption of 3D visualization and accelerate the standardization of digital processes.
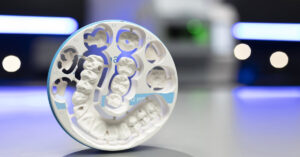
Components: base frame, positioning template and reduction jigs
Base frame serves as the indexing support for the entire stacked structure and can be fixed to remaining teeth, the mucosa or directly to bone using anchoring pins; its mechanical stability is critical for accurate transfer of coordinates during subsequent manipulations and for photogrammetric control of drilling.
Positioning template is designed for accurate transfer of the base frame position to the supporting anatomy and is usually removed after frame fixation, leaving a fixed platform for the installation of reduction modules and osteotomy sleeves.
Reduction template visualizes the volume of bone resection and forms the restorative space — this is important when determining implant vertical position and the volume of osteoplasty; osteotomy guides, fixed to the frame, control the trajectory, depth and spatial position of implants via metal sleeves or guiding channels.
Materials and manufacturing: methods and clinical significance
The choice of material and manufacturing method is influenced by the required stiffness, accuracy and biocompatibility — constructions made of titanium or cobalt‑chrome alloys provide increased stiffness and resistance to deformation, polymer photopolymers and PMMA are applicable for working guides and provisional elements, additive technologies allow rapid production of complex geometries with high accuracy.
Clinical implications include the influence of guide deformation on the cumulative error of implant positioning and the necessity of validating materials and manufacturing processes to ensure reproducibility; laboratory cooperation and quality control of CAD/CAM stages are mandatory elements.
Clinical illustration: maxillary treatment and digital cooperation
The case of a 66‑year‑old patient demonstrates the integration of preoperative CBCT planning, intraoral scanning and AI‑assisted segmentation for the assessment of anatomy and calculation of restorative space, with additional implants in positions 16, 13, 11, 22 and 23 planned to ensure transverse stability in the full‑arch protocol.
Practical implementation included the use of selective transparency in the software to correlate coronal and root anatomy with the bone volume, verification of screw access trajectories by merging IO‑scans with CBCT and the pre‑fabrication of a provisional prosthesis — all of which reduced operative time and increased the predictability of primary fixation.
Advantages and barriers to adoption
Advantages include increased surgical accuracy due to indexed elements, improved integration of surgical and prosthetic stages, simplification of immediate loading protocols and the possibility of full transfer of the digital plan to the clinic; barriers are the complication of digital planning, increased manufacturing costs, the need for laboratory support and the risk of cumulative error with imperfect indexing.
Recommendations for clinical practice — development of reproducible protocols, interdisciplinary cooperation between surgeons, prosthodontists and technicians, regular validation of manufacturing chains and monitoring of clinical outcomes through prospective studies and registration databases.
Conclusion
Stackable modular surgical guides demonstrate a trend toward transforming modern implantology into an integrated system based on the exchange of knowledge, digital technologies and clinical cooperation; for broad and safe clinical implementation, standardization, an evidence base and educational initiatives aimed at forming a professional culture focused on predictability and quality of treatment are necessary.
We use cookies to improve website performance, analyze traffic, and personalize content. You can accept all cookies or customize their use. Learn more in our Cookie Policy.
Functional
Always active
Technical storage or access is strictly necessary for the legitimate purpose of making possible the use of a particular service expressly requested by the subscriber or user, or solely for the purpose of carrying out the transmission of a message over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
Technical storage or access used solely for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
Technical storage or access is necessary to create user profiles for the purpose of sending advertising or to track a user across a website or multiple websites for similar marketing purposes.